Early Membran Rupture
In order for the baby to have normal bodily functions, growth and development and to be able to move comfortably, amniotic fluid is necessary. This fluid which is surrounded by membranes called amnion and chorion is dynamic fluid having very important functions during pregnancy.
The amniotic fluid protects the baby from external trauma, makes it possible to move easily, enables respiratory system development and keeps the heat at a steady temperature. Amniotic membranes specifically protect the baby from microorganisms which might pass through the vagina and cervix and go up.
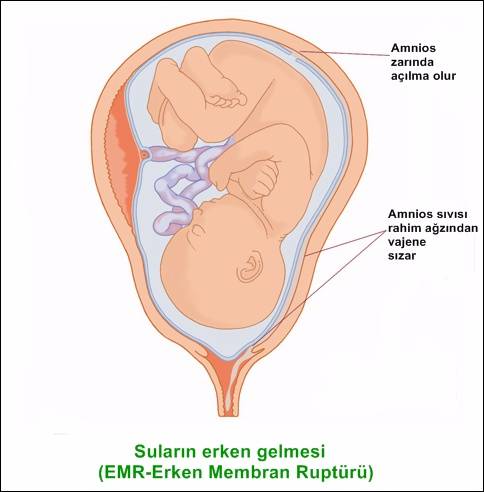
What is Early Membran Rupture (Premature Rupture Of Membranes) ?
When the amnion/amniotic membrane ruptures, and thus, water breaks early, before labour starts this is called early membrane rupture/premature rupture of membranes. With the rupture of the amnion membrane the filter mechanism that prevents the passage of germs/microorganisms from the outside world to the baby is lost. If the amniotic membrane is ruptured before the 37th week, it is called premature early membrane rupture/preterm premature rupture of membranes (PPROM). Premature rupture of membranes is one of the leading causes of premature labour.
It is observed in about 10% of all pregnancies. Candidate mothers mention of a fluid which is suddenly discharged from the vagina. However, this discharge might not always be very distinct and might be in small amounts.
There are various reasons; however, generally, infections are held responsible. Especially, urinary tract infections and vaginal infections are on top of the list.
Other reasons include cervical failure, multiple pregnancies, polyhydramnios, lack of mother’s nutrition and smoking.
Diagnosis starts with suspicion. When the mother-to-be suspects water break, ultrasound scan and an examination is done. During a speculum examination, done to observe the cervix (vaginal entry), amniotic fluid discharge can be seen. On suspicion, by doing a pH evaluation using litmus paper, it can be determined whether the fluid is amniotic or cervical mucus. Then again, with the ultrasound scan the amount of amnion fluid surrounding the baby is examined.
When PROM is diagnosed, depending on the week of pregnancy, overall physical examination, blood tests and the overall condition of the baby, the treatment is planned. The most important complication regarding PROM is premature labour. Usually, within 24 hours, after the water breaks, labour starts.
Another serious condition that might cause problems both for the mother and the fetus is chorioamniotic infection (intrauterine infection). After the early membran rupture each passing moment increases the risk of infection. In about 9-15% of all PROMs chorioamniotic infection occurs. This condition shows symptoms and is diagnosed by fever, fewer baby movements, pain in the abdominal wall, bad smelling vaginal fluid discharge and increase in the number of white cells in blood analysis. When chorioamniotic infection is diagnosed, antibiotic treatment in proper doses and spectrum should immediately be started and pregnancy ended as soon as possible.
In PROM the treatment method involves either to wait and see or terminate the pregnancy. The observation method of PROM varies from one patient to the other. The method of treatment is decided depending on the week of pregnancy, how long PROM has been lasting, baby’s biophysical conditions, mother’s overall physical examination results and more importantly whether there is infection or not.
If birth is already due or near and if the baby’s lung development will not pose a threat, it is advised not to wait for too long for labour. By using labour induction (oxytocin) labour can be initiated. If C-section is required, then pregnancy is ended under antibiotic suppression. If the pregnancy is between 28-34 weeks and if conditions do not pose a risk for the mother and the baby, some time can be gained during antibiotics treatment. Sometimes the rupture on the amnion may be very small and the body can repair itself during the observation-wait period.
If pregnancy is less than 26 weeks, it is difficult to make the decision whether to wait or end the pregnancy because a long amount of time is required for the baby to develop. Thus, the risk of infection is high. Additionally, if oligohydramnios lasts for a long time, it will have a negative effect on the baby’s lung developmentt. That’s why, in such cases, termination of pregnancy might be considered after consulting the issue with the parents.